This is Part 1 of the Symptoms to Sources series, drawn from Test Double's original research report, Symptoms to Sources: Biggest Software Challenges for Healthcare in 2026.
- You are here: Healthcare software teams keep fixing symptoms: Real problems run deeper
- Legacy systems and delivery pressure: Symptoms healthcare tech teams keep treating
- The root causes healthcare teams overlook: Siloed data and misaligned priorities
- How to shift focus from symptoms to build stronger healthcare software systems
Healthcare organizations battle internal inefficiency, complex regulatory frameworks, and interoperability challenges daily. When systems can't talk to one another, engineering and product teams spend more time managing technology than improving care.
Your gut instinct is probably to blame the technical problems—slow software, confusing dashboards, siloed data, or manual workarounds—so you spin up your next software project, bug resolution, or product feature.
But when foundational processes, communication, and data governance are fractured, even the best tools and busiest developers can't create consistent value. These same organizations often struggle to find ways to use advances in technology to achieve greater outcomes for their patients.
AI is making this worse, not better. Data governance was bad before—now it's limiting teams' ability to adopt new technology at all. Companies have always struggled to focus on projects and features that truly generate business value. Now we're seeing AI raise the failure rate over 90%. Regulatory challenges were prevalent before. Now it's a nightmare of trying to suss out what data is flowing where. Untangle one thread and you hit another knot.
At Test Double, we see this cycle in healthcare organizations all the time, so we take a different approach. Instead of addressing symptoms, we uncover root causes across the entire software lifecycle while solving hard business problems and enabling cultural change. We leave your healthcare IT, engineering, and product teams better than we found them.
When solving IT symptoms keeps teams sick
You're back in the doctor's office for the third time this month. Pounding headache, endless nausea, and numbing fatigue persist—undeterred by three separate medications prescribed to ease each symptom.
Looked at together, these symptoms could point to a variety of medical issues—COVID, diabetes, or mononucleosis—each requiring a very different treatment plan. But by analyzing and treating each symptom separately from the whole, your physician misses the mark completely, and you continue to live in discomfort.
Healthcare tech teams fall into this same trap. Whether it's a formal product and software engineering team or a product-like function within marketing, strategy, clinical operations, or IT, teams find themselves solving symptom after symptom: fixing bugs, filling gaps, and rolling out new features. They're spinning the wheel faster and faster without moving outcomes or the business forward.
The same pattern plays out across the broader healthcare ecosystem. Healthcare technology, systems, and applications are long overdue for legacy modernization and innovation—but it needs to be strategic rather than tactical.
"Healthcare is very inefficient. There's a lot of manual calling and talking to people, pushing papers, and faxing things. It's unnecessarily challenging. But, there are lots of technical opportunities underlying everything we do. We sit on troves of data about our customers and patients. How can we take all of that amazing data to help our patients be well?"
— Sara Saldoff, Head of Product Management and User Experience at OhioHealth
The current state of healthcare software
Technology offers healthcare providers the promise of increased efficiency, cost savings, and additional resources to provide better patient care. Patients, meanwhile, gain greater access to health records, more holistic support, and convenient channels for collaborating with providers and offices.
Yet this high-demand industry is rife with challenges. Healthcare systems are responsible for compliantly managing confidential patient data under the strictest data privacy laws. Software must work seamlessly, with application availability and interoperability vital to success.
Digital transformation is advancing unevenly across regions, tools, and practices—creating inequity in care, inefficient data siloes, and clinician burnout. With patient care outcomes in the balance, the stakes couldn't be higher.
Three macro trends shaping health IT in 2026
Three macro trends shape the next phase of health IT and how patients and providers understand, measure, and collaborate on healthcare outcomes.
Stagnated patient adoption of health IT
Health tech empowers patients with convenient, direct access to their health records and healthcare providers. Over the past decade, patients embraced digitization of personal healthcare, but use cases have stagnated—revealing opportunities to expand digital care.
Between 2012 and 2024, patient adoption of health IT grew dramatically. Among individuals who used online medical records, 90% viewed results online and 79% used digital technology to message providers.
Patient portals have become the norm for making appointments, downloading information, reviewing clinical notes, and correcting medical records. But there remains a pressing need to move beyond basic access toward deeper online engagement.
Poor UI/UX design is frequently at the crux of lackluster engagement. When patient portals are buggy or difficult to navigate, users get frustrated. When patients are forced to re-enter identifying information (as required by HIPAA regulations), they feel inconvenienced. As a result, patients only log in to complete a pressing task—like viewing test results—but don't explore the portal further.
Adding to this, many product teams feel pressure to release feature after feature but often fail to address patients' real needs. This combination—poor usability and fewer features focused on end users' experience—gives patients little incentive to use health tech to its full potential.
Inequitable engagement and access across healthcare systems
By 2024, only 56% of hospitals enabled patients to import their records from other organizations into their patient portal, and just 62% allowed patients to submit patient-generated data (PGD) such as tracking weight or blood glucose levels.
These are prime use cases for patients to engage more directly in their health journey and build a more useful personal health profile.
Further widening the gap, hospitals with fewer resources often lack the capabilities to enable app-based patient access to health information. Hospitals that used electronic health record (EHR) developers other than the market leaders see lower adoption rates—70% for app access, compared to 92% for EHR market leaders.
Part of the challenge lies with the EHRs themselves. Many providers avoid upgrading or expanding their EHR platforms because they're expensive, inflexible, and complex. These barriers make it difficult for hospitals to innovate or connect seamlessly with external systems.
To reach higher levels of patient engagement, healthcare systems must achieve true interoperability and improve resource equity.
Fragmented interoperability in healthcare data exchange
Interoperability sits at the center of health IT challenges. Healthcare vendors pursue a shared goal: building data standardization and APIs to support interconnectedness so that anybody can walk into a physician's office and access a complete, 360-degree picture of their health.
But building truly interoperable, scalable solutions brings both technical and strategic challenges in an environment shaped by policy, diverse user needs, and the inequitable market power of dominant EHRs.
Despite these hurdles, adoption of interoperable standards is accelerating. Between 2018 and 2023, hospitals and clinicians steadily expanded their use of interoperable exchange methods. National networks saw the fastest growth, with 48% of hospitals using interoperable exchanges for sending data and 46% for receiving in 2023—up from 20% and 18%, respectively, in 2018.
Insert chart: Interoperability adoption growth from 2018–2023 showing national network exchange rates. A simple line or bar chart showing the increase from ~20% to ~48% for sending and ~18% to ~46% for receiving.
Even as exchange methods evolve, true interoperability is hugely influenced by the market power of a few major vendors. Clinicians used more than 193 different certified developers in 2023, but Epic dominates the space—62% of clinicians reported at least one certified health tech product from Epic. Cerner Corporation, Athena Health, eClinicalWorks, and NextGen Healthcare were comparatively minor mentions, and 188 alternative developers fell into an Other category.
"When we think about interoperability and data standardization more broadly, it's not something we can solve privately by one organization–it's more significant. And, when we talk about access to data and what's required to be compliant with legislation, there's an outsized amount of power and impact that the larger players have. We've seen a lot of startups that either lose traction or fold entirely because they didn't anticipate the playing field or the power of some of those big players."
— Kiley Blake, Senior Vice President of Product and Information Technology at KODE Health
Because of this concentration of power, APIs and standards like the Fast Healthcare Interoperability Resources (FHIR) requirements act as essential guardrails to keep data flowing across healthcare systems, EHRs, and apps.
Many hospitals balance a mix of standards-based and proprietary APIs to meet different needs. About 80% of hospitals use APIs to enable apps to write to EHRs and read data, but only 33% of those connections use standards-based APIs. Roughly half of hospitals use APIs to access data outside the EHR, and just 17% rely on standards-based APIs for that purpose. This mix shows the tension between innovation and standardization—complicating reliability, security, and support.
Together, the data shows an advancing but fragmented interoperability landscape. For engineering and product teams, building and supporting interoperable products means working across local HIEs, national networks, proprietary systems, and legal frameworks like TEFCA—each with its own standards, policies, and data quality requirements.
While national policy pushes for more unified exchange, product and engineering teams operate in gray areas. They're left to navigate competing standards, vendor dominance, and legacy system integration while maintaining the highest levels of compliance, consent, security, and usability.
Key industry shifts affecting healthcare engineering teams
On top of these macro challenges, the healthcare industry is in perpetual evolution. Three industry shifts that engineering and product teams—and their healthcare customers—must navigate right now:
HTI-4 Final Rule and what it means for engineering teams
The ASTP/ONC HTI-4 Final Rule formalized changes to medical prescription policies, effective October 2025. These changes aim to make prescription costs more transparent, speed up access to care, advance interoperability, and reduce administrative burden through upgraded APIs, revised standards, and enhanced EHR workflows.
The impacts for engineering and product teams include real-time prescription benefit checks requiring integration of formulary and cost data into EHR workflows, electronic prior authorization (FHIR-based) requiring HL7 FHIR-based APIs to query payer requirements, and updated e-prescribing standards meaning upgrades to prescribing modules while ensuring compatibility with legacy systems.
Tariffs disrupting healthcare vendor logistics and tech budgets
Tariffs driven by the federal government's trade policy shift are disrupting medical supply chains, from consumer goods to manufacturing and pharmaceuticals. These policies evolve so quickly that reliable figures are difficult to cite. For healthcare systems, navigating the resulting uncertainty and making sound strategic decisions is increasingly difficult.
One thing is certain: healthcare systems will feel the pain in increased costs and shortages for equipment, medicines, resources, and supplies. Many hospitals and medical offices will have to move funds to cover immediate needs and postpone critical technology modernization projects—sacrificing future efficiency and better patient care in the process.
Cybersecurity threats and the cost of outdated healthcare systems
Healthcare systems and vendors must safeguard against cybersecurity incidents to protect patient safety and data confidentiality. The 2024 cybersecurity incident impacting Change Healthcare, a subsidiary of UnitedHealth Group, demonstrated exactly how high the stakes are.
With Change Healthcare responsible for processing 15 billion healthcare transactions—touching one in three patient records—the consequences of the ransomware attack were far-reaching. The American Hospital Association found that 74% of surveyed hospitals reported direct patient care impact, including delays in authorizations for medically necessary care, and 33% reported the attack disrupted more than half of their revenue.
Outdated systems often mean vulnerabilities and security flaws that are easily exploited. Preventative maintenance offers proactive protection against growing cybersecurity risks. Planned upgrades need to be a routine process—not a reactive crisis—to keep systems secure and minimize disruption.
Where healthcare technology leaders are investing in 2026
We asked healthcare executives to compare their investment priorities for 2025 against 2024. We expected significant increased investments in AI, and survey results backed this up: 84% of healthcare leaders increased AI spending in 2025 and plan to do the same in 2026.
But we also see a bump in strategy and innovation, particularly planned for 2026. Only 5% of healthcare teams are decreasing this investment, 37% are keeping the same level, and 58% are increasing the budget.
.jpg)
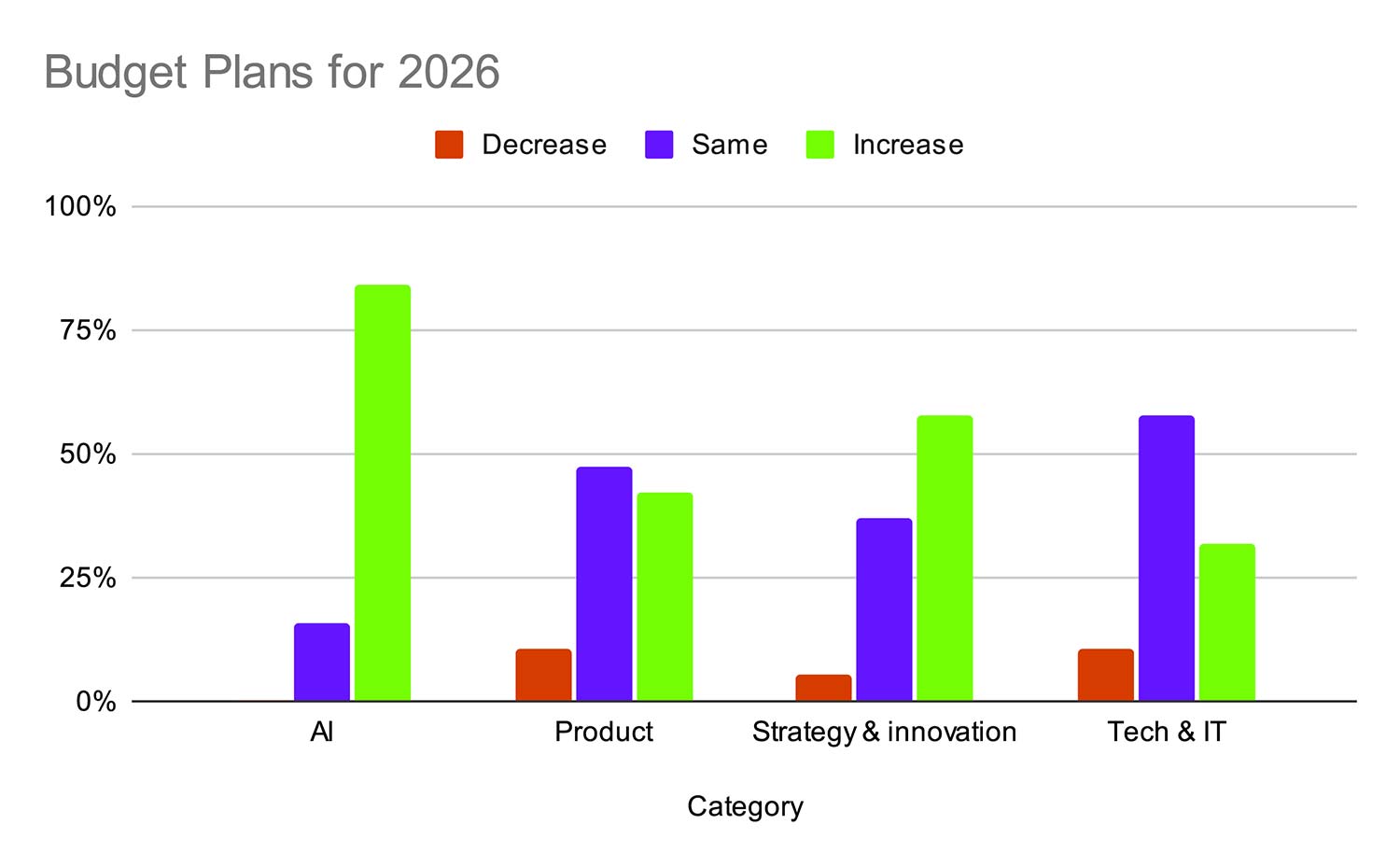
This data suggests that AI hype is very real, with healthcare teams feeling pressure to invest in the biggest shift in health tech right now. But they likely aren't seeing the return yet, with AI projects underperforming or failing to generate business value.
When we dug deeper into the specific technology projects health teams are investing in, 84% cited AI and ML as the tech projects they spent the most on in 2025, and 76% spent heavily on workflow and process automation. Cybersecurity landed in sixth place, with only 11% making it the key investment.

Under financial pressure to innovate while being as lean and efficient as possible, healthcare systems are grappling with tradeoffs. Pouring money into AI and automation without a strong research and development budget or a team with hands-on experience in these projects is a recipe for disaster.
A consultant experienced in both strategy and technology makes all the difference. A consultant can help healthcare organizations prioritize initiatives against defined business objectives—launching more successful AI and automation projects and optimizing spend so budget is freed up for other crucial categories like cybersecurity.
Frequently asked questions about healthcare software challenges in 2026
Why are healthcare AI projects failing at higher rates than other industries?
Healthcare AI projects face a compounding problem: the data governance gaps that existed before AI are now the primary bottleneck. AI models require clean, standardized, well-governed data to produce reliable outputs—and most healthcare organizations don't have that foundation in place. When you layer in HIPAA compliance requirements, fragmented EHR ecosystems, and the sheer volume of unstructured clinical data, the technical lift to get AI projects into production is significantly higher than in industries with fewer regulatory constraints. Our survey found 84% of healthcare leaders are increasing AI spend, but without addressing underlying data quality and governance issues first, that investment is unlikely to generate meaningful business value.
How does the HTI-4 Final Rule affect engineering teams that aren't directly building EHR products?
Even if your team doesn't build EHR software, HTI-4 has downstream impacts. The rule's FHIR-based electronic prior authorization requirements mean any system that touches prescriptions, insurance claims, or care authorization workflows will need to support new API standards. If your product integrates with EHRs—whether for scheduling, billing, patient engagement, or data analytics—your engineering team will need to update those integration points. The updated NCPDP SCRIPT standards also affect e-prescribing modules, which ripple into pharmacy platforms, telehealth apps, and clinical decision support tools. Teams that haven't mapped their integration dependencies against HTI-4 requirements risk compliance gaps and broken workflows.
Why did cybersecurity rank so low in healthcare IT investment priorities despite high-profile breaches?
Our survey found cybersecurity landed in sixth place for technology investment priorities, with only 11% of respondents naming it their top spend—despite incidents like the 2024 Change Healthcare breach. This disconnect likely reflects a few realities: AI and automation carry strong board-level pressure to invest; cybersecurity is often viewed as a cost center rather than a value driver; and many organizations treat security as a maintenance line item rather than a strategic investment. The risk is that teams defer proactive security work in favor of more visible initiatives—until a breach forces reactive, expensive remediation that displaces other priorities entirely.
What does "true interoperability" actually require beyond FHIR compliance?
FHIR compliance is necessary but not sufficient. True interoperability requires standardized data models (not just standardized APIs), consistent data governance practices across participating organizations, shared consent and identity management frameworks, and—critically—organizational willingness to share data rather than treating it as a competitive moat. The technical side involves maintaining multiple exchange methods (local HIEs, national networks, proprietary connections, and TEFCA-aligned frameworks) simultaneously. For engineering teams, this means building and maintaining integrations across systems with different standards, policies, and data quality requirements—while keeping compliance, consent, and security airtight.
What comes next in this series
This is the landscape healthcare product and engineering leaders are navigating: stagnated patient adoption, fragmented interoperability, rising cybersecurity threats, shifting regulations, and intense pressure to invest in AI—often without the strategic clarity to ensure those investments pay off.
If your organization is at one of these inflection points—navigating a scaling decision, a major modernization, or a strategic technology bet—the macro trends above aren't just industry context. They're the environment your next investment decision has to survive in.
In Part 2 of this series, we dig into the specific symptoms healthcare technical teams keep addressing—tech debt, legacy rewrites, and delivery pressure—while deeper problems persist underneath.
- You are here: Healthcare software teams keep fixing symptoms: Real problems run deeper
- Legacy systems and delivery pressure: Symptoms healthcare tech teams keep treating
- The root causes healthcare teams overlook: Siloed data and misaligned priorities
- How to shift focus from symptoms to build stronger healthcare software systems
Read the full report: Symptoms to Sources: Biggest Software Challenges for Healthcare in 2026
Know a leader in healthcare who cares about these things? Share the survey with them so we can expand our findings.
Cathy Colliver is Head of Marketing at Test Double, holds an M.B.A., and has expertise across strategy, brand, content, and marketing ops at startups, mid-size companies, and enterprise across software, healthcare insurance benefits, automotive, media, marketing solutions, and theatre.